The Government pledged to eliminate adult mental health out of area (OOA) placements by the end of March 2021, but it still hasn't happened yet. Peter Saunders explores why a consistent reduction has been difficult to sustain, despite the action taken by providers to date.
Contents
In this review, we've used publicly available data from MHSDS submissions to analyse inappropriate out of area (OOA) placements, to quantify the direct costs for trusts, highlight the scale of inappropriate OOA placements, and explore some of the challenges faced by healthcare systems in reducing them.
We also reflect on the opportunity for ICBs, providers, and system partners to promote collaborative practices across systems to improve care pathways with a focus on GIRFT (Getting it Right First Time) principles.
Analysis: the current status of inappropriate out of area placements
The number of inappropriate OOA placements that ended during the May 2022-April 2023 reporting period was 4,235. When we compare the monthly positions, there were 170 more active inappropriate OOA placements at the end of April 2023 (720), compared to the end of April 2022 (550).
Over half of inappropriate OOA placements (57%) were more than 100 km from a service user’s home (period May 2022 to April 2023), with 77% of inappropriate placements lasting 15 nights or more, and 46% lasting for 31 or more nights, over the same reporting period.
The primary diagnosis data (April 2023) show that most admissions to inappropriate OOA placements were categorised as service users ‘in crisis’ (39%) or experiencing ‘recurrent or ongoing psychosis’ (25%) .
The NHS spent £134 million is direct costs last year (May 2022 - April 2023) on inappropriate OOA placements. 88% of this spend was because of lack of available beds. We should also be mindful of the uncosted burden on health, social care, and society at large through harm experienced by a person being placed many miles from home. This includes increased distress as a result of separation from family and familiar care networks, as well as the impact on recovery rates and step-down to community care. Examples of the OOA placement key performance metrics that could be used to inform indirect costs include:
number of inappropriate OOA placements that result in readmission < 28days post-discharge
recording of the total length of stay for a service-user placed OOA – this would be cumulative length of stay accounting for the episode of care out of area as well as the subsequent 'in area' length of stay (including ward transfers) required for reassessment or further treatment prior to discharge.
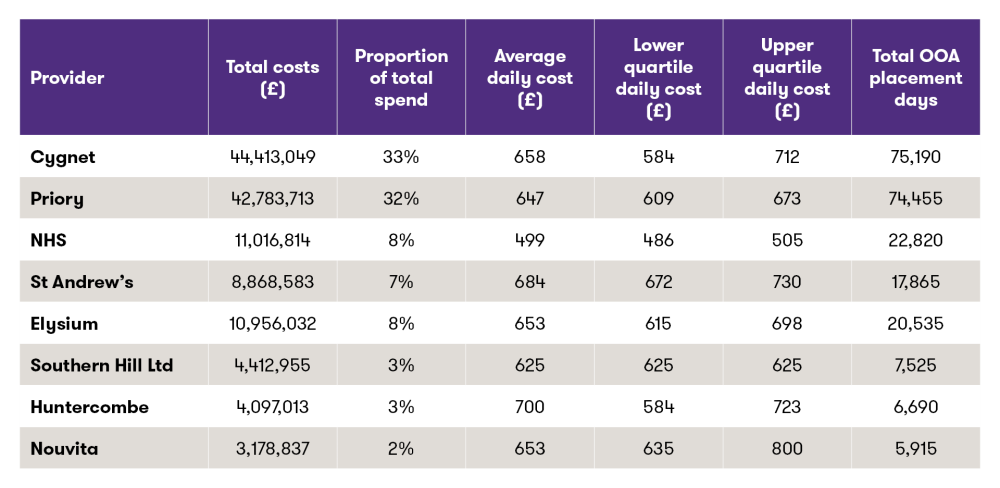
Not only do inappropriate OOA placements continue to place a significant cost burden on the NHS, but we found that over two thirds of that spend is with two main independent providers: Priory (£44.4 million) and Cygnet (£42.8 million). Average daily rates for inappropriate OOA placements ranged from £499 for NHS providers to £700 for the Huntercombe group, however, this variation is caveated as the data doesn't indicate the type of inpatient provision, for example, the cost of specialist care beds.
Furthermore, the data shows that there's a variance in lower and upper quartile daily costs across the providers. Considering the significant cost burden on the NHS it should be possible to work with Cygnet and the Priory to agree a national tariff for adult mental health acute and psychiatric intensive care unit (PICU) beds.
Source: NHS digital
Figure 1 shows total spend by inappropriate OOA placement provider (May 2022-April 2023) and the variation in daily cost rates across providers.
Challenges: four factors driving inappropriate OOA placements
The NHS long-term plan delivered increased funding for mental health services to improve access and care for children, adults, and older adults by £2.3 billion per annum by 2023/24. However, despite this investment, timely access to community, acute, and urgent care continues to be challenging. Providers report that demand is increasing for all mental health services and that complexity is also increasing.
It's important to place the current state of inappropriate OOA placements in the broader context of mental health and social care challenges, government action, and investment made to-date. There are four factors driving this general demand for mental health support.
Prolonged social isolation combined with the cost of living crisis are having real consequences for our most vulnerable communities in terms of their mental and physical health.
Children and adolescents are experiencing increasing rates of anxiety and depression, resulting in school absences and higher demand for mental health services. One-in-five children were reported as persistently absent post-COVID-19 (Department for Education figures 2022/2023).
The rise in state pension and increased waits for access to healthcare services are forcing more people out of work. There's a strong correlation between long-term physical ill-health (eg, chronic pain and cardiovascular disease) and mental ill-health.
Many mental health teams carry significant vacancies, impacting their capacity to respond to increased demand and enable timely access to care. The ongoing doctors' strikes have also increased waiting lists and extended waiting times for physical and mental healthcare. The NHS long term workforce plan stated that the demand for mental health support will increase faster than other areas of healthcare: 4.4% a year. This would mean that total mental health nursing shortfall will reach 15,800 FTEs in 2036/37. There's an ambitious plan to increase training places for mental health nursing by 93% to more that 11,000 places by 2031/32.
It's important to recognise that timely assessment and time to first treatment for those encountering mental health illness is key. If access is difficult, mental health conditions can worsen and lead to increased demand for crisis, acute, and urgent care services. There's also an adverse impact on families and carers in supporting service users while waiting for support.
Solutions
Solutions: how can inappropriate OOAs placements be reduced?
Within the context of overwhelming demand across mental health services nationally, we believe there are three key enablers to reduce inappropriate OOA placements for acute and urgent care services:
1 Capacity
Aligning demand and capacity within existing services
2 Demand
A collaborative MDT approach between systems to meet rising demand across care pathways with a focus on early intervention initiatives
3 Patient flow
Streamlining patient flow through efficient discharge planning and timely post-discharge support in community and primary care
Collaboration across systems and system partners is the essential element playing through remedial action to reduce OOA placements for acute and urgent services. It's not solely an acute and urgent issue. The causal factors for rising inpatient demand are complex and multifactorial and can only be addressed by sharing resource and capacity across systems. For example, funding for specialist housing placements and underfunding of local authorities creates financial and bureaucratic challenge, delaying patient flow, and impacting patient outcomes.
Action planning to reduce inappropriate OOA placements
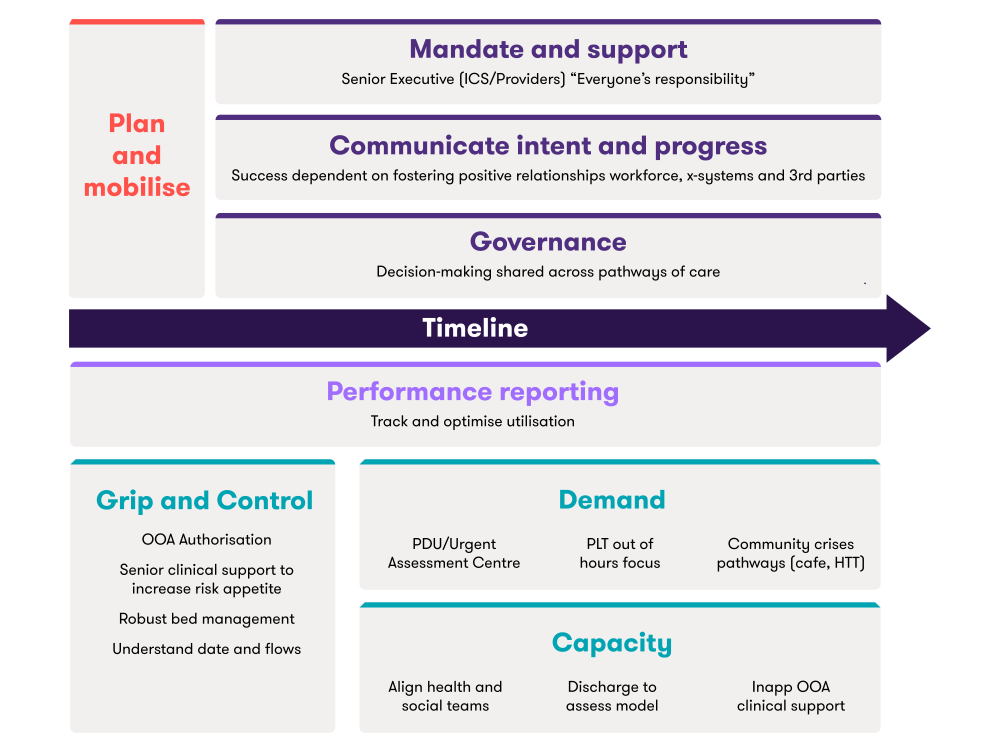
Our Best Practice Collaborative Group has enabled providers to share strategies for tackling inappropriate OOA placements. The most important component which helped to address rising inappropriate OOA placements was the appreciation and communication of shared responsibility across system partners along the care pathways (figure 2). The collaborative group felt that initial ‘grip and control’ - strong leadership and access to performance data was essential in scaffolding effective decision making. In this initial phase urgent on the ground action was also cited as key: strengthening the approvals process (governance) and robust bed management policy and practice.
Moving forward collaboration across system partners was deemed as vital to develop sustainable action plans focused on improving patient flow, releasing capacity, and optimising earlier intervention. Participants also emphasised the importance of having senior clinical leads in supporting gatekeeping teams 24/7, to help manage risk safely and effectively. Inpatient stays are essential for some service users, but for others the view was that often pressure exerted by systems and processes result in inappropriate inpatient stays and burgeoning demand for acute and PICU beds.
Figure 2 summarises the approach to reducing inappropriate OOA placements resulting from the initial best practice collaborative session.
The causal factors of inappropriate out of area placements are multi-factorial and complex. They extend beyond the operational remit of acute and urgent care services. Getting the messaging right was key to enthuse, inform, and augment the impact of our collaborative initiatives which have helped to drive down inappropriate out of area placements. The message that this was ‘everyone’s responsibility’ was reinforced in all our communications to unify the call to action across all systems and partners.
Vanessa Devlin, Chief Operating Officer, Birmingham and Solihull Mental Health Foundation Trust
How can change be delivered?
Leadership and governance
Proactive collaboration to help address increased demand for acute and urgent services should be supported by strong senior leadership across health and social care systems. An appreciation and acknowledgement that inappropriate OOA placements are everyone’s responsibility is also vital. Leaders are responsible for owning this message and supporting others to deliver the action needed to improve the impact of inappropriate OOA placements on services and service users.
One healthcare provider explained that having local authority executives (director of adult social care and the director of strategy) on the executive board had helped with decision making and embedded integrated working. This arrangement had also helped with negotiations and implementation of mental health capacity solutions with private providers and the local authority, as well as harmonised values and vision to deliver holistic interventions to improve service user outcomes as early as possible.
Collaboration
Development of cross-system partnerships and collaborative teams across independent providers, police, ambulance services, social care, VCSEs, and health organisations have proven highly effective in reducing inappropriate OOA placements.
One provider explained that acute and urgent care teams were working collaboratively with community colleagues on the same site wherever possible. To this end, one large provider collaborative is hoping to rollout place-based collaborative mental health teams. The discussion group felt that providers who support populations that are more spread out and denser would probably benefit more from a place-based structure.
Understanding data
Ensuring that data is robust to support monitoring and tracking of inappropriate OOA placements, that patient records are available 24/7 for all gatekeeping teams and that patient records are shared with independent providers to facilitate step-up and step-down from OOA units.
The group shared that daily oversight of service users in independent provider beds was crucial to expedite return to in area beds. Dedicated discharge teams were established to focus on this task. Providers agreed that more evidence is needed to determine the level of crisis provision in community which is optimal for a population.
Managing demand - gatekeeping
Ensuring that gatekeepers are aware of the alternative therapeutic pathways and have access to patient records to help inform clinical risk assessment and avoid inappropriate referrals.
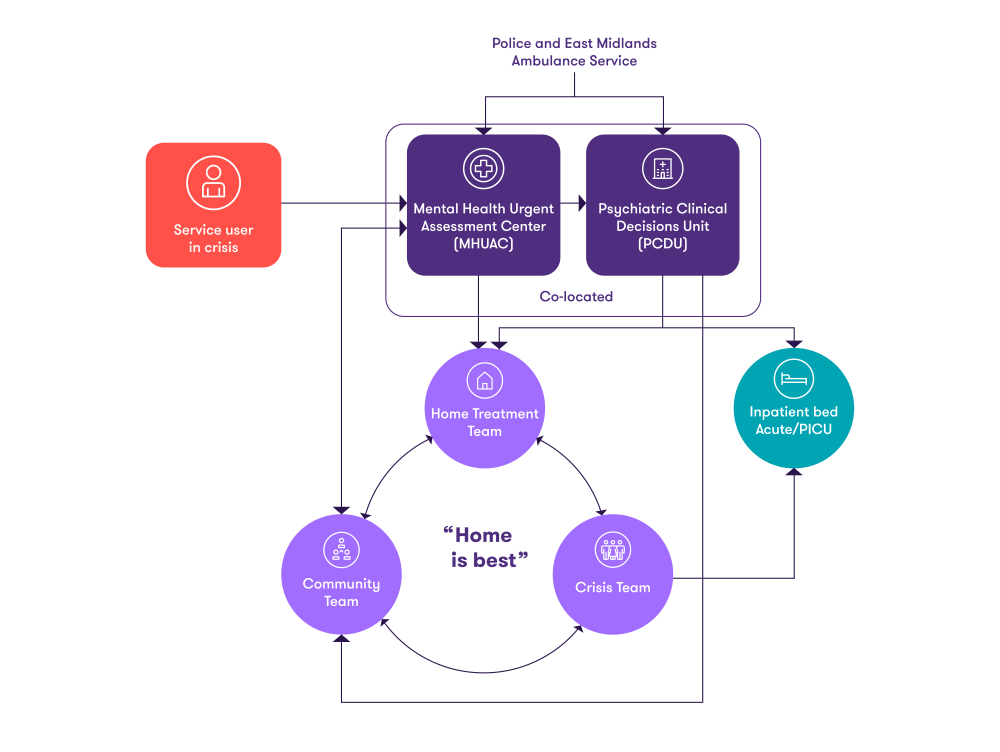
One of the trusts who participated in the best practice collaborative, Lincolnshire Partnership NHS Foundation Trust, was happy to share their own gatekeeping model, which we've illustrated in this diagram.
Diagram 1: overview of Lincolnshire Partnership NHS Foundation Trust care pathway
The success of this access and delivery model is predicated on:
out of hours provision is the same as in-hours aligned to demand
senior psychiatric doctors assess and hold the risk at the admission entry points in-hours and out-of-hours
the crisis team has a single point of access for primary and community team referrals
Psychiatric Clinical Decisions Unit (PCDU) and crisis teams are the gatekeepers for inpatient beds
the Mental Health Urgent Assessment Centre (MHUAC) is sited alongside the PCDU – it provides staffing and an appropriate environment to help manage the needs of service users in mental health crisis; avoiding admission to the acute emergency department
Optimising existing capacity
Optimising the use of out-of-hours services and independent provision while reducing the length of stay can significantly improve patient flow and the service user experience of care.
The North West bed bureau works across Mersey care, Cheshire and Wirral, Greater Manchester and Pennine to exploit the capacity in the independent sector for the benefit of service users who need access to more local bed, where there's no in area capacity. All providers agreed that a focus on timely step-down from acute and urgent beds is key to facilitate patient flow. Discharge collaboration hubs (health and social care workforce) offer one solution. The challenge continues to be funding for specialist care and housing, and rehab capacity for some within the independent sector caused by reduced risk appetite to meet some complex service user needs.
Workforce skill-mix
Incorporating peer navigators, social prescribers, refreshing acute day hospital support and working with neighbourhood networks to help strengthen the support network for service users, families and carers to help step-down from inpatient beds effectively and safely, or to support them in avoiding an inpatient stay.
New pressures are accelerating transformation in health and social care
Learn more about how our Health and social care services can help you
Inappropriate OOA placements continue to be a pressing and costly issue for providers. The distress caused is immeasurable for service users and families, too many are placed many miles away from home at a time when they are at their most vulnerable. Strong leadership, cross-system collaboration, strengthened gatekeeping functions and processes, and data-driven decision making all help to reduce inappropriate OOA placements. The best practice collaboration group continues to support and learn from each other, sharing knowledge and experience around mental healthcare issues to improve service user experience and outcomes.
The Public Sector Finance Leaders Barometer is a nationwide pulse check of the pressures, priorities and sentiment shaping local government finance. Compiled from the insights of Section 151 officers and finance directors, it provides a data‑rich view of how leaders are navigating 2026, a year defined by financial constraints, regulatory complexities and rising demand.
On the 3rd July 2025, the Labour government published its 10-year health plan for the NHS, setting out its vision to transform how healthcare is delivered across England. For health tech innovators, this is not just a policy, it’s a game-changing opportunity. Our experts Will Rose and Jessica Sandercock outline the key details of the plan and its impact on Health Tech in the UK.